General: Agitation and Insomnia: Increased restlessness, agitation, anxiety and insomnia, especially shortly after initiation of treatment, have been associated with treatment with bupropion. In 3 placebo-controlled clinical trials of seasonal affective disorder with Wellbutrin XL, the incidence of agitation, anxiety and insomnia are shown in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patients in placebo-controlled trials of MDD with Wellbutrin SR, the sustained-release formulation of bupropion, experienced agitation, anxiety and insomnia as shown in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
In clinical studies of MDD, these symptoms were sometimes of sufficient magnitude to require treatment with sedative/hypnotic drugs.
Symptoms in these studies were sufficiently severe to require discontinuation of treatment in 1% and 2.6% of patients treated with 300 and 400 mg/day, respectively, of bupropion sustained-release tablets and 0.8% of patients treated with placebo.
Psychosis, Confusion and Other Neuropsychiatric Phenomena: Depressed patients treated with bupropion have been reported to show a variety of neuropsychiatric signs and symptoms, including delusions, hallucinations, psychosis, concentration disturbance, paranoia and confusion. In some cases, these symptoms abated upon dose reduction and/or withdrawal of treatment.
Activation of Psychosis and/or Mania: Antidepressants can precipitate manic episodes in bipolar disorder patients during the depressed phase of their illness and may activate latent psychosis in other susceptible patients. Wellbutrin XL is expected to pose similar risks.
Altered Appetite and Weight: In 3 placebo-controlled clinical trials of seasonal affective disorder with Wellbutrin XL, the percentage of patients with weight gain or weight loss are shown in Table 4. (See Table 4.)
Click on icon to see table/diagram/image
In placebo-controlled studies of MDD using Wellbutrin SR, the sustained-release formulation of bupropion, patients experienced weight gain or weight loss as shown in Table 5. (See Table 5.)
Click on icon to see table/diagram/image
In studies conducted with the immediate-release formulation of bupropion, 35% of patients receiving tricyclic antidepressants gained weight, compared to 9% of patients treated with the immediate-release formulation of bupropion. If weight loss is a major presenting sign of a patient's depressive illness, the anorectic and/or weight-reducing potential of Wellbutrin XL should be considered.
Allergic Reactions: Anaphylactoid/anaphylactic reactions characterized by symptoms eg, pruritus, urticaria, angioedema and dyspnea requiring medical treatment have been reported in clinical trials with bupropion. In addition, there have been rare spontaneous post-marketing reports of erythema multiforme, Stevens-Johnson syndrome and anaphylactic shock associated with bupropion. A patient should stop taking Wellbutrin XL and consult a physician if experiencing allergic or anaphylactoid/anaphylactic reactions (eg, skin rash, pruritus, hives, chest pain, edema and shortness of breath) during treatment.
Arthralgia, myalgia and fever with rash and other symptoms suggestive of delayed hypersensitivity have been reported in association with bupropion. These symptoms may resemble serum sickness.
Cardiovascular Effects: In clinical practice, hypertension, in some cases severe, requiring acute treatment, has been reported in patients receiving bupropion alone and in combination with nicotine replacement therapy. These events have been observed in both patients with and without evidence of preexisting hypertension.
Data from a comparative study of the sustained-release formulation of bupropion (Zyban sustained-release tablets), NTS, the combination of sustained-release bupropion plus NTS and placebo as an aid to smoking cessation suggest a higher incidence of treatment-emergent hypertension in patients treated with the combination of sustained-release bupropion and NTS. In this study, 6.1% of patients treated with the combination of sustained-release bupropion and NTS had treatment-emergent hypertension compared to 2.5%, 1.6% and 3.1% of patients treated with sustained-release bupropion, NTS, and placebo, respectively. The majority of these patients had evidence of preexisting hypertension. Three patients (1.2%) treated with the combination of Zyban and NTS and 1 patient (0.4%) treated with NTS had study medication discontinued due to hypertension compared to none of the patients treated with Zyban or placebo. Monitoring of blood pressure is recommended in patients who receive the combination of bupropion and nicotine replacement. There is no clinical experience establishing the safety of Wellbutrin XL in patients with a recent history of myocardial infarction or unstable heart disease. Therefore, care should be exercised if it is used in these groups. Bupropion was well tolerated in depressed patients who had previously developed orthostatic hypotension while receiving tricyclic antidepressants, and was also generally well tolerated in a group of 36 depressed inpatients with stable CHF. However, bupropion was associated with a rise in supine blood pressure in the study of patients with CHF, resulting in discontinuation of treatment in 2 patients for exacerbation of baseline hypertension.
Hepatic Impairment: Wellbutrin XL should be used with extreme caution in patients with severe hepatic cirrhosis. In these patients, a reduced frequency and/or dose is required. Wellbutrin XL should be used with caution in patients with hepatic impairment (including mild to moderate hepatic cirrhosis) and reduced frequency and/or dose should be considered in patients with mild to moderate hepatic cirrhosis.
All patients with hepatic impairment should be closely monitored for possible adverse effects that could indicate high drug and metabolite levels (see Dosage & Administration, Warnings, and Pharmacology: Pharmacokinetics under Actions).
Renal Impairment: There is limited information on the pharmacokinetics of bupropion in patients with renal impairment. An inter-study comparison between normal subjects and patients with end-stage renal failure demonstrated that the parent drug C
max and AUC values were comparable in the 2 groups, whereas the hydroxybupropion and threohydrobupropion metabolites had a 2.3- and 2.8-fold increase, respectively, in AUC for patients with end-stage renal failure. A 2nd study, comparing normal subjects and patients with moderate to severe renal impairment (GFR 30.9±10.8 mL/min) showed that exposure to a single 150 mg dose of sustained-release bupropion was approximately 2-fold higher in patients with impaired renal function while levels of the hydroxybupropion and threo/erythrohydrobupropion (combined) metabolites were similar in the 2 groups. Bupropion is extensively metabolized in the liver to active metabolites, which are further metabolized and subsequently excreted by the kidneys.
Wellbutrin XL should be used with caution in patients with renal impairment and a reduced frequency and/or dose should be considered as bupropion and the metabolites of bupropion may accumulate in such patients to a greater extent than usual. The patient should be closely monitored for possible adverse effects that could indicate high drug or metabolite levels.
Information for Patients: Prescribers or other health professionals should inform patients, their families and their caregivers about the benefits and risks associated with treatment with Wellbutrin XL and should counsel them in its appropriate use.
Patients should be advised of the following issues and asked to alert the prescriber if these occur while taking Wellbutrin XL.
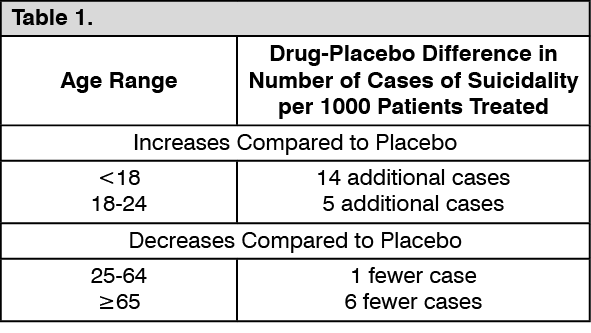
Clinical Worsening and Suicide Risk: Patients, their families and their caregivers should be encouraged to be alert to the emergence of anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, mania, other unusual changes in behavior, worsening of depression and suicidal ideation, especially early during antidepressant treatment and when the dose is adjusted up or down. Families and caregivers of patients should be advised to look for the emergence of such symptoms on a day-to-day basis, since changes may be abrupt. Such symptoms should be reported to the patient's prescriber or health professional, especially if they are severe, abrupt in onset or were not part of the patient's presenting symptoms. Symptoms such as these may be associated with an increased risk for suicidal thinking and behavior and indicate a need for very close monitoring and possibly changes in the medication.
Neuropsychiatric Symptoms and Suicide Risk in Smoking Cessation Treatment: Although Wellbutrin XL is not indicated for smoking cessation treatment, it contains the same active ingredient as Zyban which is approved for this use. Patients should be informed that quitting smoking, with or without Zyban, may be associated with nicotine withdrawal symptoms (including depression or agitation) or exacerbation of preexisting psychiatric illness. Furthermore, some patients have experienced changes in mood (including depression and mania), psychosis, hallucinations, paranoia, delusions, homicidal ideation, aggression, anxiety and panic, as well as suicidal ideation, suicide attempt and completed suicide when attempting to quit smoking while taking Zyban. If patients develop agitation, hostility, depressed mood or changes in thinking or behavior that are not typical for them, or if patients develop suicidal ideation or behavior, they should be urged to report these symptoms to their healthcare provider immediately.
Patients should be made aware that Wellbutrin XL contains the same active ingredient found in Zyban, used as an aid to smoking cessation treatment and that Wellbutrin XL should not be used in combination with Zyban or any other medications that contain bupropion hydrochloride (eg, Wellbutrin SR, the sustained-release formulation, and Wellbutrin, the immediate-release formulation).
Patients should be told that Wellbutrin XL should be discontinued and not restarted if they experience a seizure while on treatment.
Patients should be told that any central nervous system-active drug like Wellbutrin XL may impair the ability to perform tasks requiring judgment or motor and cognitive skills. Consequently, until they are reasonably certain that Wellbutrin XL do not adversely affect their performance, they should refrain from driving an automobile or operating complex, hazardous machinery.
Patients should be told that the excessive use or abrupt discontinuation of alcohol or sedatives (including benzodiazepines) may alter the seizure threshold. Some patients have reported lower alcohol tolerance during treatment with Wellbutrin XL. Patients should be advised that the consumption of alcohol should be minimized or avoided.
Patients should be advised to inform physicians if they are taking or plan to take any prescription or over-the-counter drugs. Concern is warranted because Wellbutrin XL and other drugs may affect each other's metabolism.
Patients should be advised to notify physicians if they become pregnant or intend to become pregnant during therapy.
Patients should be advised to swallow Wellbutrin XL whole so that the release rate is not altered. Do not chew, divide or crush tablets.
Patients should be advised that they may notice in their stool something that looks like a tablet. This is normal. The medication in Wellbutrin XL is contained in a non-absorbable shell that has been specially designed to slowly release drug in the body. When this process is completed, the empty shell is eliminated from the body.
Laboratory Tests: There are no specific laboratory tests recommended.
Drug Abuse and Dependence: Controlled Substance Class: Bupropion is not a controlled substance.
Humans: Controlled clinical studies of bupropion (immediate-release formulation) conducted in normal volunteers, in subjects with a history of multiple drug abuse and in depressed patients showed some increase in motor activity and agitation/excitement.
In a population of individuals experienced with drugs of abuse, a single dose of bupropion 400 mg produced mild amphetamine-like activity as compared to placebo on the Morphine-Benzedrine Subscale of the Addiction Research Center Inventories (ARCI) and a score intermediate between placebo and amphetamine on the Liking Scale of the ARCI. These scales measure general feelings of euphoria and drug desirability.
Findings in clinical trials, however, are not known to reliably predict the abuse potential of drugs. Nonetheless, evidence from single-dose studies does suggest that the recommended daily dosage of bupropion when administered in divided doses is not likely to be especially reinforcing to amphetamine or stimulant abusers. However, higher doses that could not be tested because of the risk of seizure might be modestly attractive to those who abuse stimulant drugs.
Animals: Studies in rodents and primates have shown that bupropion exhibits some pharmacologic actions common to psychostimulants. In rodents, it has been shown to increase locomotor activity, elicit a mild stereotyped behavioral response and increase rates of responding in several schedule-controlled behavior paradigms. In primate models to assess the positive reinforcing effects of psychoactive drugs, bupropion was self-administered IV. In rats, bupropion produced amphetamine-like and cocaine-like discriminative stimulus effects in drug discrimination paradigms used to characterize the subjective effects of psychoactive drugs.
Carcinogenesis, Mutagenesis, Impairment of Fertility: Lifetime carcinogenicity studies were performed in rats and mice at doses up to 300 and 150 mg/kg/day, respectively. These doses are approximately 7 and 2 times the maximum recommended human dose (MRHD), respectively, on a mg/m
2 basis. In the rat study, there was an increase in nodular proliferative lesions of the liver at doses of 100-300 mg/kg/day (approximately 2-7 times the MRHD on a mg/m
2 basis); lower doses were not tested. The question of whether or not such lesions may be precursors of neoplasms of the liver is currently unresolved. Similar liver lesions were not seen in the mouse study, and no increase in malignant tumors of the liver and other organs was seen in either study.
Bupropion produced a positive response (2-3 times control mutation rate) in 2 of 5 strains in the Ames bacterial mutagenicity test and an increase in chromosomal aberrations in 1 of 3
in vivo rat bone marrow cytogenetic studies.
A fertility study in rats at doses up to 300 mg/kg/day revealed no evidence of impaired fertility.
Use in Children: Safety and effectiveness in the pediatric population have not been established (see Clinical Worsening and Suicide Risk under Warnings). Anyone considering the use of Wellbutrin XL in a child or adolescent must balance the potential risks with the clinical need.
Use in the Elderly: Of the approximately 6,000 patients who participated in clinical trials with bupropion sustained-release tablets (depression and smoking cessation studies), 275 were ≥65 years old and 47 were ≥75 years old. In addition, several hundred patients ≥65 years participated in clinical trials using the immediate-release formulation of bupropion (depression studies). No overall differences in safety or effectiveness were observed between these subjects and younger subjects. Reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
A single-dose pharmacokinetic study demonstrated that the disposition of bupropion and its metabolites in elderly subjects was similar to that of younger subjects; however, another pharmacokinetic study, single- and multiple-dose, has suggested that the elderly are at increased risk for accumulation of bupropion and its metabolites (see Pharmacology: Pharmacokinetics under Actions).
Bupropion is extensively metabolized in the liver to active metabolites, which are further metabolized and excreted by the kidneys. The risk of toxic reaction to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection and it may be useful to monitor renal function (see Renal Impairment as previously mentioned and Dosage & Administration).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image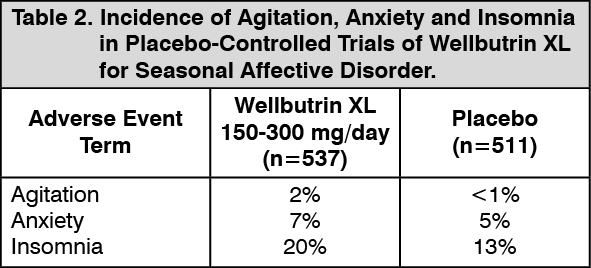 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image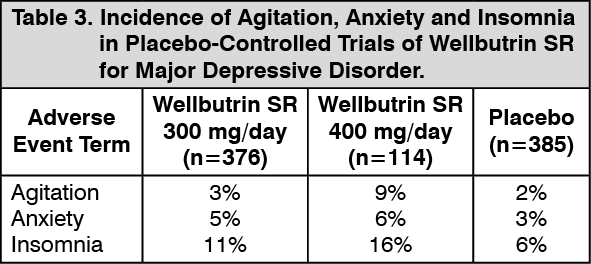 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image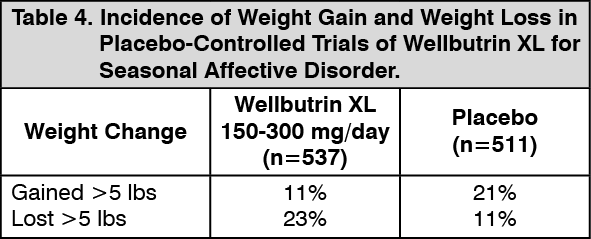 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image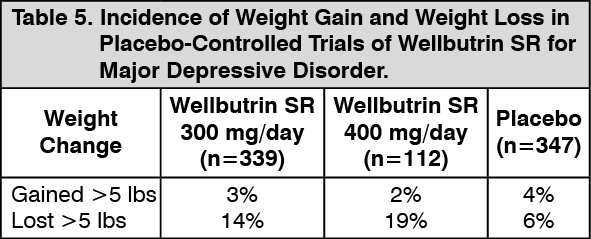 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image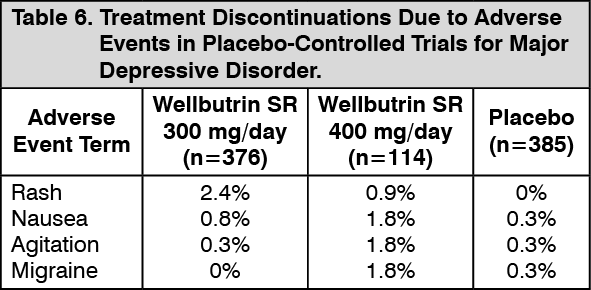 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image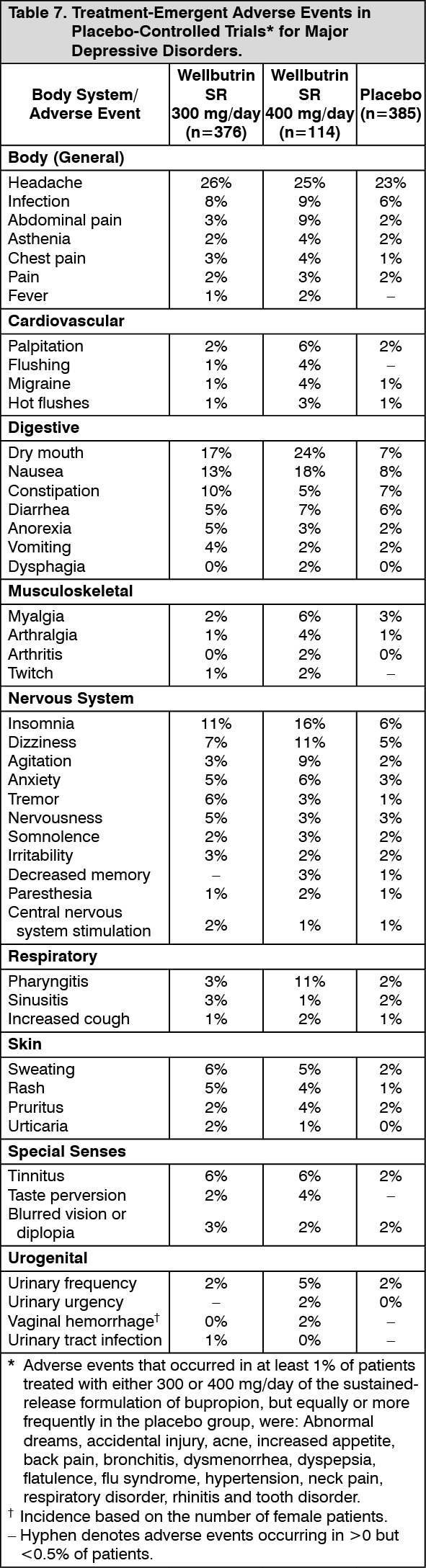 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image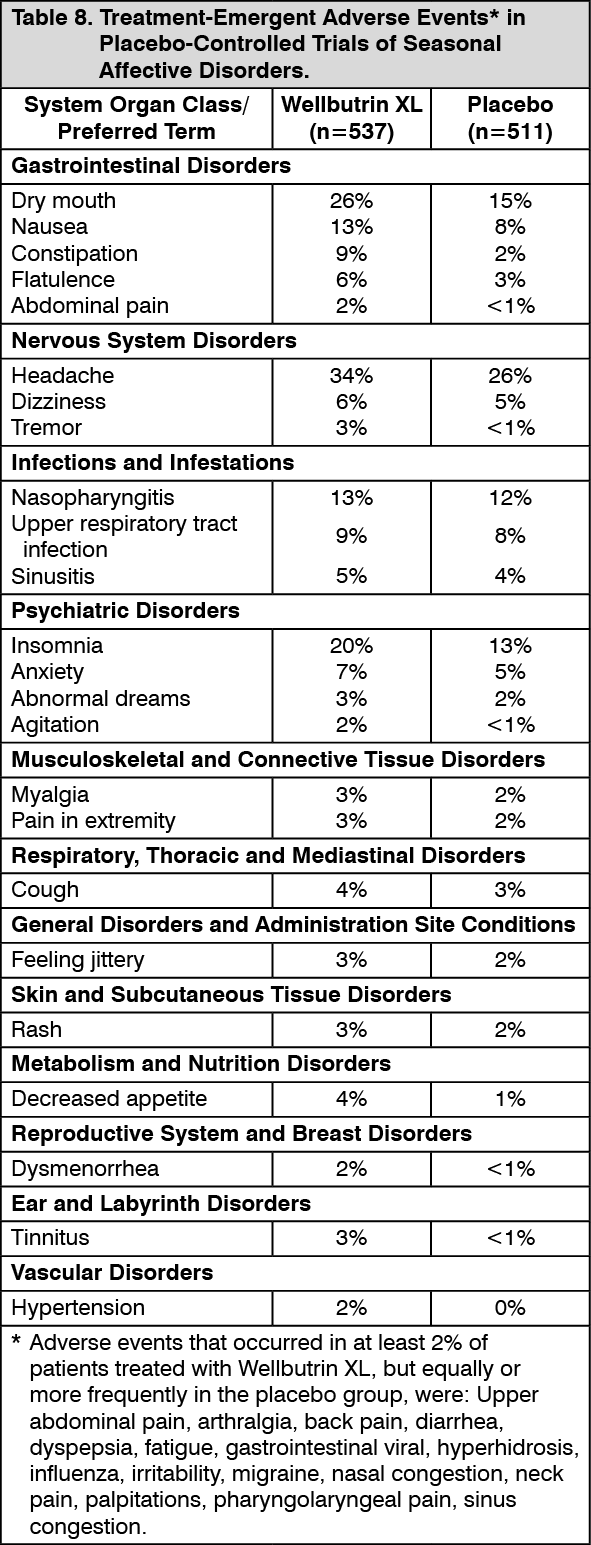 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
